Clinical Documentation Improvement Workflow: A Step-by-Step Guide to Precision and Compliance
Published: 06/04/2026 Updated: 06/05/2026
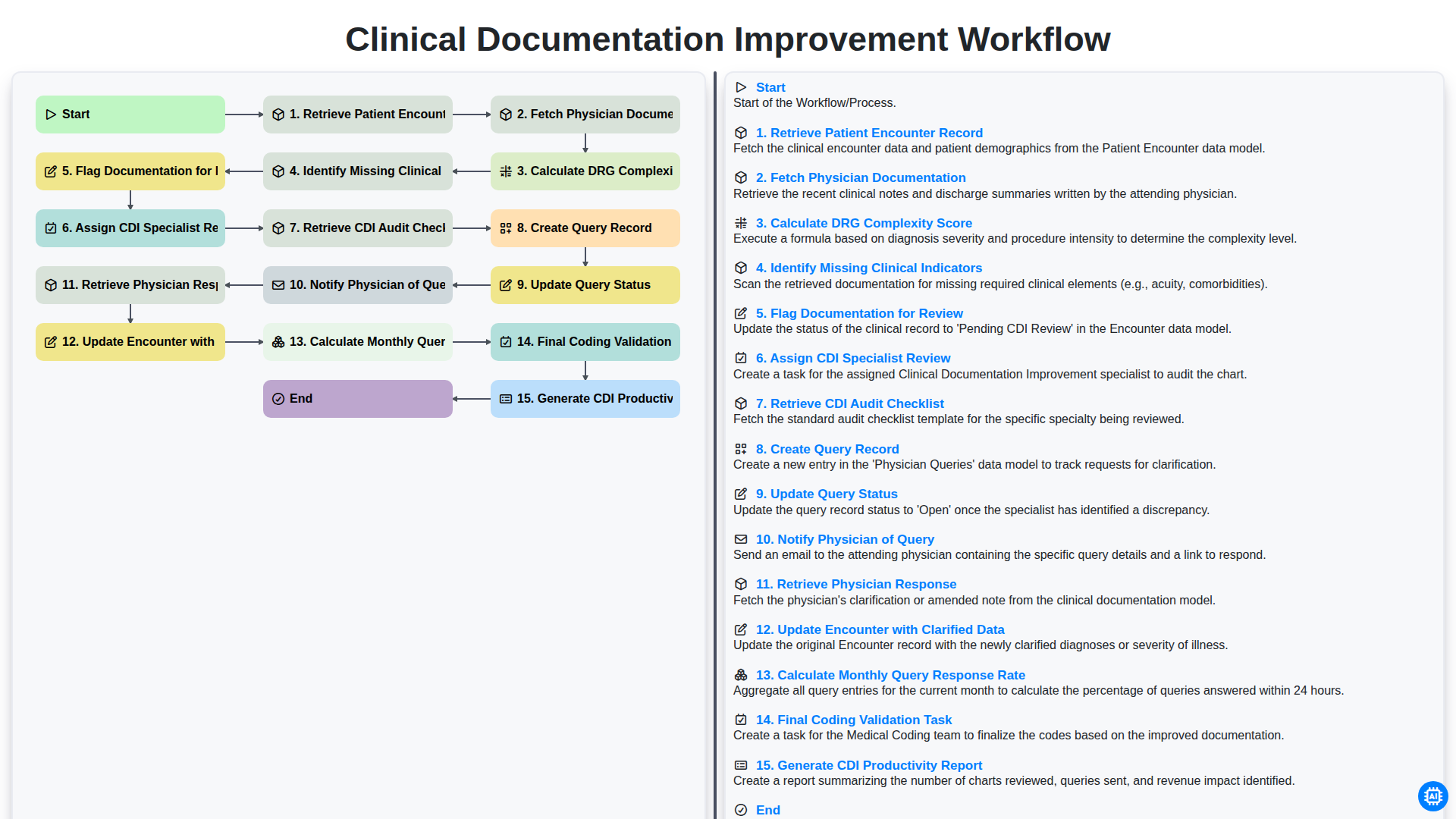
Table of Contents
- Introduction to Clinical Documentation Improvement (CDI)
- Phase 1: Data Retrieval and Initial Assessment
- Step 1: Retrieving Patient Encounter Records and Physician Documentation
- Step 2: Analyzing DRG Complexity and Clinical Indicators
- Phase 2: Identifying Documentation Gaps and Flagging Discrepancies
- Step 3: Initiating the CDI Specialist Review Process
- Phase 3: The Query Management Lifecycle
- Step 4: Implementing CDI Audit Checklists and Query Creation
- Step 5: Tracking Query Status and Physician Notification
- Step 6: Managing Physician Responses and Data Clarification
- Phase 4: Finalizing the Encounter and Coding Validation
- Step 7: Updating Records and Performing Final Coding Validation
- Phase 5: Performance Analytics and Continuous Improvement
- Step 8: Measuring Query Response Rates and CDI Productivity
- Resources & Links
TLDR: This guide breaks down the end-to-end Clinical Documentation Improvement (CDI) workflow, detailing how to streamline the process from initial record retrieval and DRG complexity calculation to physician querying and final coding validation. Learn how to implement this structured approach to ensure documentation accuracy, improve physician communication, and drive measurable productivity through automated auditing and reporting.
Introduction to Clinical Documentation Improvement (CDI)
Clinical Documentation Improvement (CDI) is a critical proactive process designed to bridge the gap between the clinical care provided to a patient and the formal medical coding that represents that care. At its core, CDI is about ensuring that the medical record is complete, accurate, and reflects the true severity of illness and complexity of the patient's condition. When documentation is precise, it allows for a more accurate representation of patient outcomes, optimizes reimbursement accuracy, and ensures compliance with regulatory standards.
In the modern healthcare landscape, a successful CDI program relies on more than just clinical expertise; it requires a structured, repeatable, and efficient workflow. A well-defined process ensures that physicians and CDI specialists are working in tandem to capture essential clinical indicators that might otherwise be overlooked. By implementing a systematic approach-from the initial retrieval of encounter records to the final validation of coding-healthcare organizations can reduce documentation gaps, minimize claim denials, and ultimately improve the integrity of the entire revenue cycle.
Phase 1: Data Retrieval and Initial Assessment
The foundation of a successful Clinical Documentation Improvement (CDI) program lies in the accuracy of the initial data collection and the precision of the preliminary analysis. The process begins with the Retrieve Patient Encounter Record step, ensuring that all relevant clinical data points are centralized for evaluation. Once the encounter is identified, the system must Fetch Physician Documentation, pulling the raw clinical notes, discharge summaries, and progress reports that serve as the primary source of truth.
With the documentation in hand, the workflow moves into a critical analytical stage. The system will Calculate DRG Complexity Score to determine the potential severity of illness and the expected resource intensity for the case. During this calculation, the engine simultaneously works to Identify Missing Clinical Indicators-scanning for gaps where clinical evidence may exist in the labs or vitals but is not explicitly documented in the narrative. Finally, any discrepancies or gaps found during this scan will Flag Documentation for Review, effectively isolating high-priority cases that require human intervention to ensure the clinical picture is complete and accurate.
Step 1: Retrieving Patient Encounter Records and Physician Documentation
The foundation of an effective Clinical Documentation Improvement (CDI) program lies in the seamless integration of data accessibility. The workflow begins with the critical first step: Retrieving Patient Encounter Records. This stage involves gathering all relevant patient data from the Electronic Health Record (EHR) to ensure the CDI team has a comprehensive view of the patient's clinical journey.
Once the encounter record is secured, the next essential action is to Fetch Physician Documentation. This involves pulling all clinical notes, discharge summaries, operative reports, and pathology results associated with the specific encounter. Accurate retrieval of this documentation is vital, as the entire downstream analysis-including complexity scoring and query generation-depends entirely on the quality and completeness of the data pulled during this initial phase. Without a thorough retrieval process, gaps in the clinical narrative may remain undetected, undermining the integrity of the entire CDI lifecycle.
Step 2: Analyzing DRG Complexity and Clinical Indicators
Once the physician's documentation has been retrieved, the core of the CDI process begins with a deep dive into the clinical data. This stage is centered on two critical analytical tasks: calculating the DRG complexity score and identifying missing clinical indicators.
The primary goal here is to move beyond simple-level documentation and determine the true acuity of the patient's condition. By applying standardized algorithms to the available data, the workflow calculates a DRG complexity score, which serves as a baseline for the expected resources required for the patient's care.
However, a score alone is not enough. The system-or the specialist-must then cross-reference the documentation against established clinical criteria to identify gaps. This involves searching for missing indicators, such as specific laboratory values, vital signs, or diagnostic evidence that would support a higher-level diagnosis. For example, if a physician documents sepsis but fails to note the associated hypotension or lactate levels, the workflow flags this as a missing clinical indicator. This proactive identification ensures that the clinical picture is complete before the record moves further into the coding stage.
Phase 2: Identifying Documentation Gaps and Flagging Discrepancies
Once the initial physician documentation has been fetched and the DRG complexity score is calculated, the workflow moves into a critical diagnostic stage. This phase focuses on bridging the gap between the raw clinical data and the specific requirements needed for accurate coding and reimbursement.
The process begins by systematically identifying missing clinical indicators-those essential elements of a patient's clinical picture, such as acuity, specificity, or secondary diagnoses, that are absent from the current record. Once these gaps are detected, the system must flag documentation for review, marking specific encounters that require closer scrutiny to ensure the severity of illness (SOI) and risk of mortality (ROM) are accurately captured.
By pinpointing these discrepancies early, the workflow transitions from passive data collection to active clinical intelligence, ensuring that no critical diagnostic detail is overlooked before the review process begins.
Step 3: Initiating the CDI Specialist Review Process
Once the system has flagged documentation gaps and identified missing clinical indicators, the workflow transitions from automated detection to human expertise. This stage is critical, as it moves the process from raw data analysis to clinical interpretation.
The process begins by assigning a CDI Specialist to the review queue, ensuring that the flagged encounter is routed to a specialist with the appropriate clinical expertise. To ensure a standardized and rigorous evaluation, the specialist then retrieves the CDI Audit Checklist. This checklist serves as the foundational guide, ensuring that every potential discrepancy-from acuity levels to specificity in diagnoses-is evaluated against established institutional standards.
With the checklist in hand, the specialist performs a deep dive into the record to determine if the identified gaps require formal intervention or if the existing documentation sufficiently supports the assigned complexity.
Phase 3: The Query Management Lifecycle
Once the initial documentation gaps are identified, the workflow transitions into the critical stage of communication and clarification. This phase, known as the Query Management Lifecycle, is where the CDI specialist bridges the gap between raw clinical data and-coded accuracy.
The process begins by formalizing the findings into a structured format. First, the system must Create a Query Record that details the specific discrepancy found during the audit. To ensure transparency and tracking, the system will automatically Update the Query Status (e.g., Open, Pending, or Answered), allowing for real-time monitoring of the physician's workload.
The next vital step is to Notify the Physician of the Query. This notification must be timely and clear, providing the necessary context so the physician can review the clinical evidence without unnecessary administrative burden. Once the physician has reviewed the case, the workflow moves to Retrieve the Physician Response, which captures the clinical clarification or additional documentation provided.
The final movement in this phase involves closing the loop. The system must then Update the Encounter with Clarified Data, ensuring that the newly provided clinical indicators are integrated into the patient record for accurate coding. To maintain oversight, the system will simultaneously Calculate the Monthly Query Response Rate, a key performance indicator (KPI) used to evaluate physician engagement and the overall efficiency of the CDI program.
Step 4: Implementing CDI Audit Checklists and Query Creation
Once a documentation gap is identified and flagged for review, the workflow shifts from detection to investigation. This stage is critical as it ensures that the CDI specialist does not rely solely on intuition, but rather on a standardized, evidence-based approach.
To maintain high-quality standards, the specialist must Retrieve the CDI Audit Checklist. This checklist serves as a roadmap, ensuring that all necessary clinical indicators-such as lab results, imaging findings, and nursing notes-are cross-referenced against the physician's initial statement. By following a structured checklist, the specialist can ensure that the clinical picture is complete before any formal communication occurs.
If a discrepancy or ambiguity is found, the next essential step is to Create a Query Record. A query is a formal request for clarification sent to the physician; it must be non-leading and clinically supported. Once the query is drafted, the specialist must Update the Query Status (e.g., Pending, Sent, or Replied) within the EHR or CDI software. This real-time tracking is vital for maintaining visibility into the documentation pipeline and ensuring that no clinical clarification falls through the cracks during the billing cycle.
Step 5: Tracking Query Status and Physician Notification
Once a documentation gap is identified and a query is initiated, the workflow moves into the critical phase of active monitoring. This stage involves two simultaneous, interconnected actions: updating the query status and notifying the physician of the query.
Effective query management relies on real-time visibility. As soon as a query is generated, the status must be updated within the CDI software to reflect that it is Pending. This ensures that the CDI specialist and the coding team have an accurate view of the current workload and can prevent duplicate efforts. Continuous updates-moving from Pending to Physician Responded or Closed-are essential for maintaining the integrity of the audit trail.
Parallel to status tracking is the notification process. For a CDI program to be successful, the communication loop must be closed quickly. Automated notifications are sent directly to the physician, alerting them to the specific encounter that requires clarification. By streamlining this notification, you reduce the time-to-response, ensuring that clinical clarifications are captured while the patient encounter is still fresh in the physician's mind. This prevents delays in the billing cycle and ensures that the final DRG assignment accurately reflects the true complexity of the patient's care.
Step 6: Managing Physician Responses and Data Clarification
Once the query has been sent, the workflow moves into the critical phase of real-time data refinement. The next essential step is to Retrieve Physician Response, as the accuracy of the entire clinical record depends on the quality of the physician's clarification. Whether the physician agrees with the query or provides supplemental clinical evidence, this information must be captured immediately to ensure the medical record reflects the true complexity of the patient's condition.
After the response is received, the workflow transitions to Update Encounter with Clarified Data. This stage is where the improvement in Clinical Documentation Improvement actually manifests; the documentation is updated to include the specific, clarified details that align the clinical narrative with the necessary coding requirements.
To ensure the loop is closed and the integrity of the process is maintained, the system must then Calculate Monthly Query Response Rate. This metric is vital for monitoring physician engagement and identifying areas where further education may be needed. Finally, the process culminates in the Final Coding Validation Task, a crucial quality control step where coders verify that the updated documentation supports the assigned codes, ensuring both compliance and optimal reimbursement accuracy.
Phase 4: Finalizing the Encounter and Coding Validation
Once the documentation has been clarified and the queries resolved, the workflow enters its critical final stage. The process moves beyond the immediate query loop to ensure that the clinical accuracy captured during the CDI process is accurately reflected in the permanent medical record.
First, the Update Encounter with Clarified Data step is executed, where the finalized physician responses and any additional clinical evidence are integrated into the patient's record. This ensures that the coding team is working with the most precise, up-to-date information available.
With the documentation solidified, the workflow transitions into the Final Coding Validation Task. During this stage, certified coders perform a final audit to ensure that the updated documentation supports the assigned codes and that the severity of illness (SOI) and risk of mortality (ROM) accurately reflect the patient's true clinical picture. This step serves as the final checkpoint to prevent coding errors and minimize downstream denials.
To conclude the cycle, the workflow shifts from individual patient care to high-level administrative oversight through two key analytical steps:
- Calculate Monthly Query Response Rate: This metric is used to evaluate physician engagement and the effectiveness of the CDI team's communication strategies.
- Generate CDI Productivity Report: This report aggregates data to assess the overall impact of the CDI program, providing stakeholders with insights into documentation accuracy, workload distribution, and the overall ROI of the CDI intervention.
By completing these final steps, the facility ensures that the entire CDI lifecycle-from initial retrieval to final validation-is a closed loop of continuous quality improvement.
Step 7: Updating Records and Performing Final Coding Validation
Once the physician has responded to the query, the workflow moves into the critical phase of data integration and finalization. The first priority is to Retrieve Physician Response and Update Encounter with Clarified Data, ensuring that the clinical nuances captured during the query process are accurately reflected in the patient's permanent medical record. This step is vital for maintaining the integrity of the clinical narrative and ensuring that the documentation supports the complexity of the care provided.
Following the documentation update, the process transitions from clinical clarification to administrative precision. The Final Coding Validation Task is executed to ensure that the updated documentation aligns perfectly with the assigned DRG. This final check serves as a quality control gate, confirming that all identified clinical indicators are properly captured before the claim is submitted. By verifying that the documentation and the code match the clinical reality, the organization minimizes the risk of denials and ensures maximized reimbursement accuracy.
Phase 5: Performance Analytics and Continuous Improvement
The final stage of an effective CDI workflow extends beyond the individual patient encounter; it focuses on macro-level oversight to ensure long-term accuracy and operational efficiency. To maintain a high standard of documentation integrity, the workflow must transition from clinical review to data-driven evaluation.
This phase begins with the Calculation of the Monthly Query Response Rate, a critical metric that measures the effectiveness of physician engagement and the clarity of the queries being issued. By analyzing how often physicians respond to queries and the nature of those responses, CDI programs can identify specific documentation gaps or areas where further physician education is required.
To ensure the integrity of the entire cycle, a Final Coding Validation Task is executed. This step serves as a quality control checkpoint, verifying that the clarified clinical indicators have been accurately translated into the final codes and that the documentation supports the assigned DRG.
Finally, all processed data is aggregated to Generate the CDI Productivity Report. This report provides stakeholders with a comprehensive view of the program's impact, tracking workload volume, query outcomes, and the overall improvement in clinical specificity. Through this continuous loop of analysis and reporting, the CDI program evolves from a reactive review process into a proactive engine for hospital-wide clinical excellence.
Step 8: Measuring Query Response Rates and CDI Productivity
To ensure the long-term success of a Clinical Documentation Improvement program, the workflow must extend beyond individual patient encounters and move into the realm of high-level analytics. Once the queries are resolved and the documentation is clarified, the final stage of the workflow shifts focus toward calculating monthly query response rates and generating CDI productivity reports.
Tracking the monthly query response rate is a vital metric for assessing the effectiveness of physician communication. By monitoring how often physicians respond to queries and the quality of those responses, CDI teams can identify patterns-such as specific departments or specialties that may require additional education or simplified query templates. A high response rate often correlates with improved clinical accuracy and reduced audit risk.
Simultaneously, the workflow culminates in the generation of CDI productivity reports. These reports serve as the pulse check for the entire CDI department, aggregating data on query volumes, physician engagement, and the impact of documentation improvements on DRG accuracy. By analyzing these metrics alongside the final coding validation tasks, healthcare organizations can transform raw documentation data into actionable insights, ensuring that the CDI program remains a value-driven component of the revenue cycle management strategy.
Resources & Links
- AHIMA (American Health Information Management Association): The primary professional organization for health information management, providing essential standards,-best practices, and regulatory guidelines for CDI professionals.
- ACDIS (Association of Clinical Documentation Integrity Specialists): A specialized resource for clinical documentation integrity professionals, offering educational tools, webinars, and industry-specific workflow optimization strategies.
- CMS (Centers for Medicare & Medicaid Services): The official source for information regarding DRG (Diagnosis Related Group) definitions, reimbursement regulations, and federal compliance standards.
- AAPC (American Academy of Professional Coders): A comprehensive resource for medical coding training and certification, useful for understanding the intersection of CDI queries and final coding validation.
- Healthcare Revenue Cycle Management Resources: Insights into how CDI workflows impact the broader revenue cycle, including productivity reporting and clinical data accuracy.
- PubMed Central (PMC): Access to peer-reviewed studies and clinical research regarding the impact of clinical documentation accuracy on patient outcomes and hospital reimbursement.
Found this Article helpful?
Healthcare Management Solution Demo
Streamlining healthcare operations and improving patient care? ChecklistGuro's Work OS platform simplifies everything from patient scheduling and billing to compliance and staff management. Enhance efficiency, reduce administrative burden, and focus on what matters most: your patients. Learn how ChecklistGuro can transform your healthcare organization!
Related Articles
The Ultimate Healthcare Patient Satisfaction Survey Checklist Template
Mastering Healthcare Inventory: Your Par Level Checklist Template
Mastering Hand Hygiene: Your Compliance Checklist Template
Protecting Patients: Your Fire Safety Checklist for Patient Areas
Your Ultimate Healthcare Construction Checklist Template
Mastering Hand Hygiene: Your Compliance Checklist Template
Your Radiology Equipment Maintenance Checklist Template

Your Ultimate Guide to Healthcare Waste Management: A Checklist Template
We can do it Together
Need help with
Checklists?
Have a question? We're here to help. Please submit your inquiry, and we'll respond promptly.